Behavioral Change is at the heart of PT

If you have been to see a physical therapy professional before, you know that this type of conservative care requires patience, commitment and time. From when you make the decision to seek care, it's an additional to-do on your list:
make appointments
attend appointments
home exercises
This multi step process can feel cumbersome and adding anything into our already busy lives can feel challenging and impossible. Oftentimes, it ends up on the pile of ‘things I'd like to change’ instead of ‘things I've changed’.
For myself, this creates a negative feedback loop where I feel bad about the things I didn’t do rather than focusing on how to change my behavior to accommodate the new habit. Maybe you can relate.
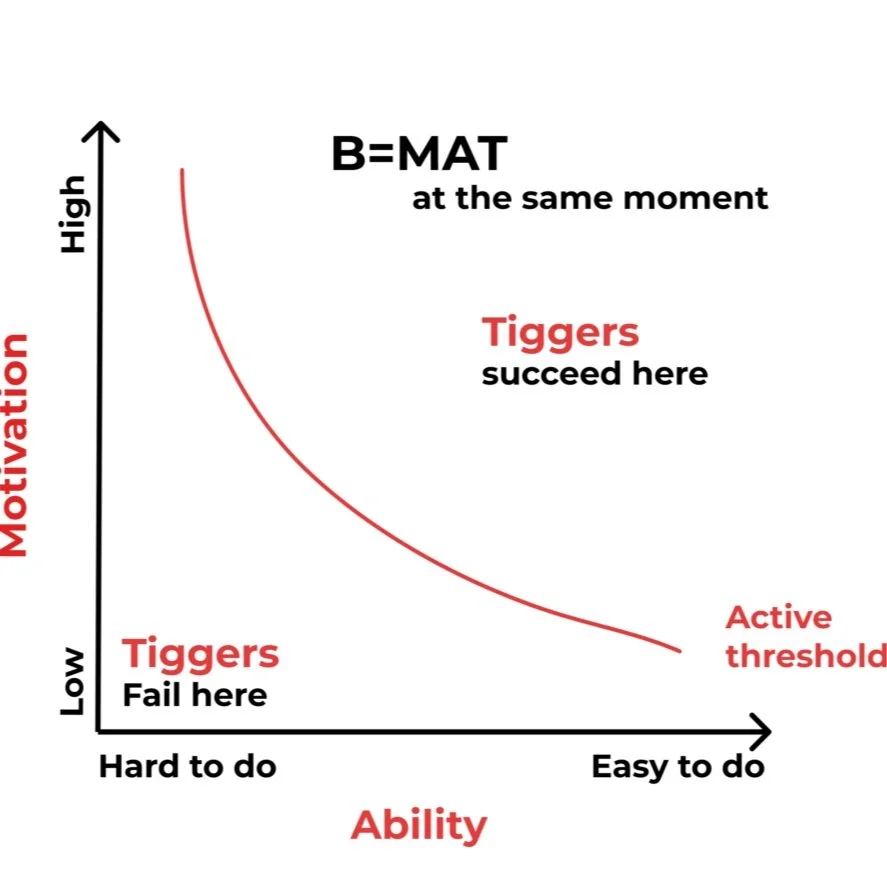
(Fogg, 2020)
So, how can we create change and actually check our home program off the list so we can feel better?
BJ Fogg, a behavioral change scientist at Stanford University developed the Fogg Behavioral Model, to explain how people can bridge the gap between what they say they want to do and what they actually do (B. Fogg, 2009). His basic premise for behavioral change relies on three factors: motivation, ability, and prompt. He explains that if all these three variables occur at the right amount at the right time, the desired behavior will occur.
As it pertains to physical therapy home exercises (the exercises you do when you are NOT with your therapist):
Motivation: your desire to alleviate your symptoms and find a solution to your problem
Ability: how capable are you of performing the exercises (includes whether the exercises are appropriately assigned and your confidence in performance without guidance)
Prompt: a cue (internal or external) that serves as a reminder for you to engage in the behavior
So how can you use this information to engage in healthy behaviors that will help you feel less pain or have less bladder leaks?
Most people seeking physical therapy already have the motivation to find some relief, so that part of the equation is covered.
Ability is determined by the relationship a patient has with their therapist. It is important to engage meaningfully with your therapist so that you are able to share your own limitations and capabilities around a home program. Maybe this includes a difficulty getting down on the floor to perform exercises or maybe even a hard limitation in time. Ask the tough questions and set boundaries so that both you and your therapist are setting expectations accordingly. Shared decision making among practitioners and patients improves outcomes(Hoffmann et al., 2022).
Prompts are a signal to the brain that something needs to happen. This will vary from person to person but the most important part of creating a prompt, also known as a cue or a trigger is pairing it with something you do daily. As an example, I have a night time routine, where every night I go into my bathroom to brush my teeth. Next to my toothbrush, on the counter is my floss. The placement of the floss next to my brush is my prompt to floss before I brush. This helps me a) remember to floss and b) lowers the barrier to me flossing. Creating a system like this helps you to start formulating a sort of habit map that guides your behavior. To translate this to physical therapy home programs, every evening after I tuck my daughter into bed, I go to my living room where I have some rehab equipment set out (foam roller, mat). I set a timer for 10 minutes and I do my routine. In this example, I have set up multiple cues– the foam roller and mat (physical cue), timing (my daughter goes to sleep every night) and a timer. It doesn’t have to be that layered, but it’s what works for me.
To find your own prompts and habit map, you can answer this questions:
After I ________, I will ________.
Make the actions small, miniscule even. Start with one exercise, one repetition. Do that for a week and see how the routine makes you feel. Maybe the next time you will want to do two for two repetitions. Each small action adds up to one big habit.
References